METABOLIC SURGERY
What is Metabolic Syndrome?
Metabolic syndrome is a bundle of
cardiometabolic risk factors that develop in common genetic and
environmental environments, characterized by large waist circumference,
high blood pressure, qualitative and quantitative disorders in blood
lipids, and high blood sugar. People with metabolic syndrome are 5 times
more likely to develop type 2 diabetes and 2 times more likely to
develop atherosclerotic cardiovascular disease than those without
metabolic syndrome.
To be diagnosed with metabolic syndrome, at least three metabolic risk factors must be present.
Table 1: Definition of metabolic syndrome
The surgical treatment of Metabolic Syndrome is called Metabolic Surgery.
In
the last half of the 20th century, experiments were conducted to see if
diseases such as high lipids and cholesterol could be treated with
surgical operations such as intestinal bypass.
In 1995, Dr. Walter
Pories and his research team published a paper suggesting that "Diabetes
in adults can be treated surgically." This article was a turning point.
In the following years, it was found that Type 2 diabetes and metabolic
disease could be treated surgically.
In 2009, "American Bariatric
Surgery Association" changed its name to "American Metabolic and
Bariatric Surgery Association", taking into account the beneficial
effects of surgical methods, especially in the treatment of Type 2
Diabetes Mellitus and metabolic syndrome.
Today, the term Metabolic Surgery is used specifically to describe procedures to treat type 2 diabetes and metabolic diseases.
Ileal Interposition
The
term ileal interposition is the process of replacing the last part of
the small intestine with the initial part. This surgery works on the
principle of deactivating the hormones that cause insulin resistance and
raising the hormone levels that increase insulin sensitivity.
Ileal
Interposition operation is a surgical treatment method developed for the
treatment of Type 2 Diabetes since the beginning. The definition of
metabolic syndrome includes Type 2 Diabetes, hypertension, high
cholesterol and triglyceride levels, and overweight.
Ileal
Interposition surgery is not an obesity surgery as a starting point. It
is an operation that aims to treat all health problems within the scope
of Metabolic Syndrome, especially Type 2 Diabetes. Therefore, obesity is
not among the criteria for ileal interposition surgery.
Ileal
Interposition surgery does not cause absorption restriction or
malabsorption. Patients who have had ileal interposition surgery start
to consume liquid food on the 3rd day after the surgery. Within six
months to 1 year, they can survive with a completely free diet and
without vitamin or mineral supplements.
Patients who are fit for
surgery usually stop all diabetes, blood pressure and cholesterol
medications they use after Ileal Interposition surgery. They are
observed in terms of the course of these diseases during the
hospitalization period after the surgery. The vast majority of patients
are discharged without using any of these drugs. In some of them, until
the metabolic effect settles, the use of drugs continue at gradually
decreasing doses for periods ranging from a few weeks to a few months,
in a controlled manner. When the measurements return to normal, the use
of all of these drugs are stopped.
The effect of weight loss is
not much due to the partially wider tube stomach, so it is beneficial
for patients who do not want to lose excess weight after surgery. Since
it brings the lower part of the small intestines directly to the stomach
and allows the food to pass directly to this area, it disables a part
of the upper small intestines, so its metabolic effects and its effect
on diabetes are quite high. The duration of surgery is longer. It
requires advanced laparoscopic surgery experience and skill. Although it
does not cause vitamin and mineral deficiency, it requires blood test
and vitamin/mineral level monitoring at regular intervals.
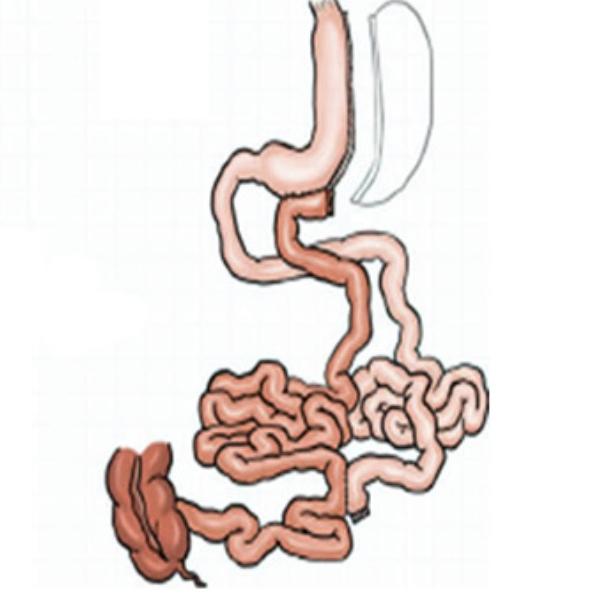
Transit Bipartition
It
is a technique introduced to the medical literature by Brazilian
surgeon Sergio Santoro. The Transit Bipartition technique is similar to
other techniques, in addition to a sleeve gastrectomy procedure, unlike
other procedures, operations on all of the ten parts of the small
intestine are performed by providing a second outlet to the lower part
of the stomach. In this way, the passage of the eaten food from all
segments of the small intestine is ensured.
In Transit
Bipartition, first of all, 100 cm is calculated from the point where the
small intestines meet with the large intestines and this part is
marked. By counting another 150 cm, the small intestine is incised at
250 cm from the junction of the small intestines with the large
intestine. The cut lower end is ligated to the stomach. The upper end is
ligated to the previously marked 100 cm. In this way, direct food entry
is provided to the last 250 cm of the small intestines. The only
important point is that approximately 1/3 of the food passes through the
duodenum, which is the natural way, and 2/3 passes through the last
part of the small intestines thanks to the newly made ligation. The
biggest advantage of this surgery is that less than 5% of patients need
iron only in the long-term. Since 1/3 of the food passes through the
normal digestive tract, more than 95% of patients can continue their
lives without the need for any supplements.
Advantages of Transit Bipartition
Less incidence of gastric sleeve leaks due to low intragastric pressure,
Failure of the gastric sleeve to expand due to low pressure in the stomach.
Since the duodenum can be accessed endoscopically, there are no problems with accessing the pancreas and bile ducts.
Continued passage and absorption of food through the entire digestive tract.
Ease of access to all parts of the digestive system endoscopically.
Access to the duodenum and bile ducts for ERCP
Less need for vitamin, mineral, iron and calcium supplements due to the protection of stomach antrum, pylorus and duodenum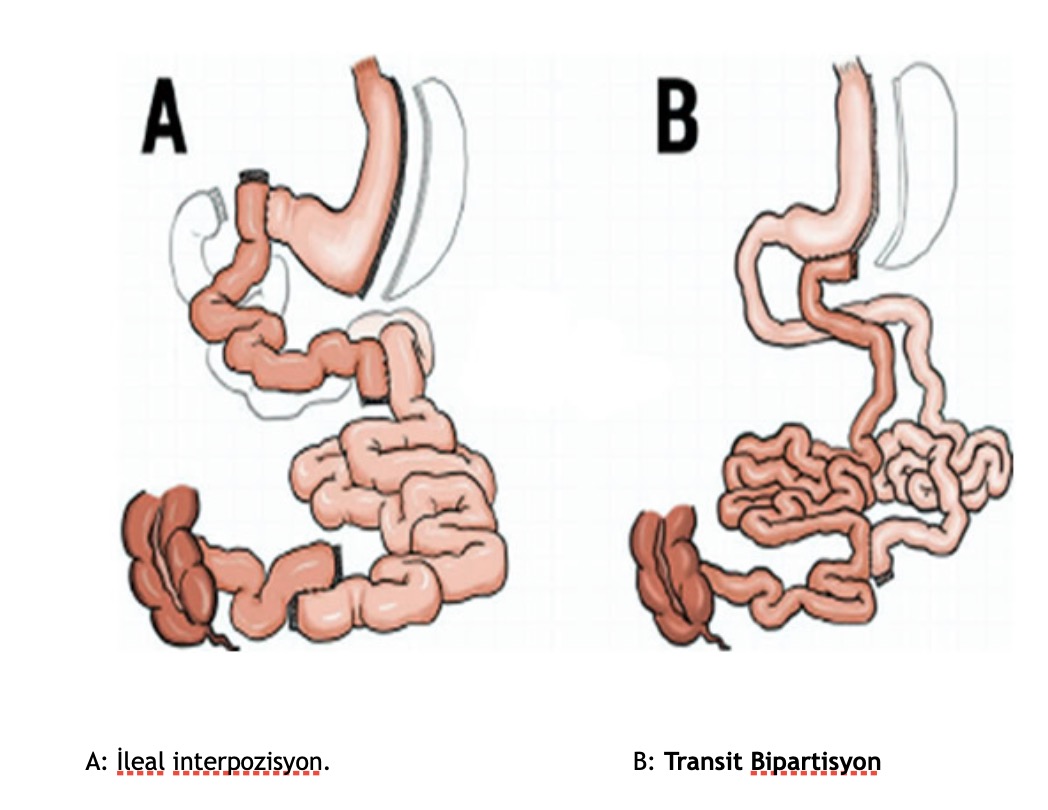
Assoc. Prof. Ahmet Tekin
General Surgeon