
WHAT IS SLEEVE GASTRECTOMY?
What is sleeve gastrectomy?
Vertical sleeve gastrectomy or
longitudinal "vertical gastrectomy" is the vertical removal of 75% of
the stomach and turning the stomach into a banana or tube shape. The
procedure is performed laparoscopically with a stapler. Laparoscopic
Sleeve Gastrectomy (LSG) is a safe and effective surgical method for
weight loss for patients with high body mass index (BMI) and high risk.
Sleeve gastrectomy is a new bariatric surgery technique that can be
performed laparoscopically and reduces the volume of the stomach. The
stomach takes the form of a tube like the continuation of the esophagus.
Since the stomach volume decreases to 25%, patients feel full when they
eat 1/4 of what they ate before. In this method, since a bypass
application is not implemented on intestines, there will be no
absorption disorder, less food causes weight loss. Sleeve gastrectomy
has emerged as a method which restricts food. However, it has been
understood that it also has metabolic effects through hormonal changes.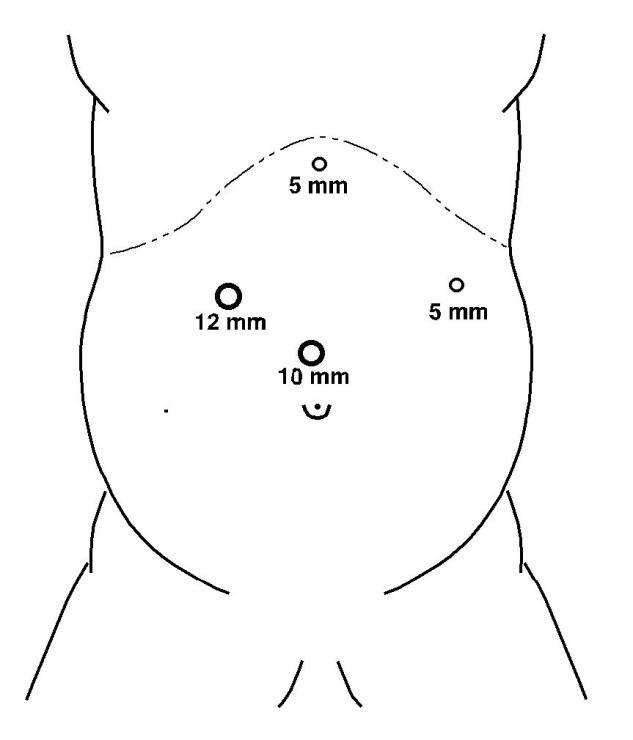
Insertion sites for laparoscopic sleeve gastrectomy
Features of sleeve gastrectomy
Sleeve gastrectomy is performed under general anesthesia using laparoscopic method using 4 insertions.
Laparoscopic sleeve gastrectomy surgery is performed with a stapler.
The stomach part separated by stapling is taken out of the abdomen through the 12 mm trocar insertion.
After laparoscopic sleeve gastrectomy surgery, the stomach volume is reduced by 75%.
It is a method with lower risk compared to other methods.
Sleeve
gastrectomy is an excellent surgical procedure for morbid obesity.
Generally, 50% of the excess weight is lost in the first 6 months after
surgery and 75% is lost within 12 months.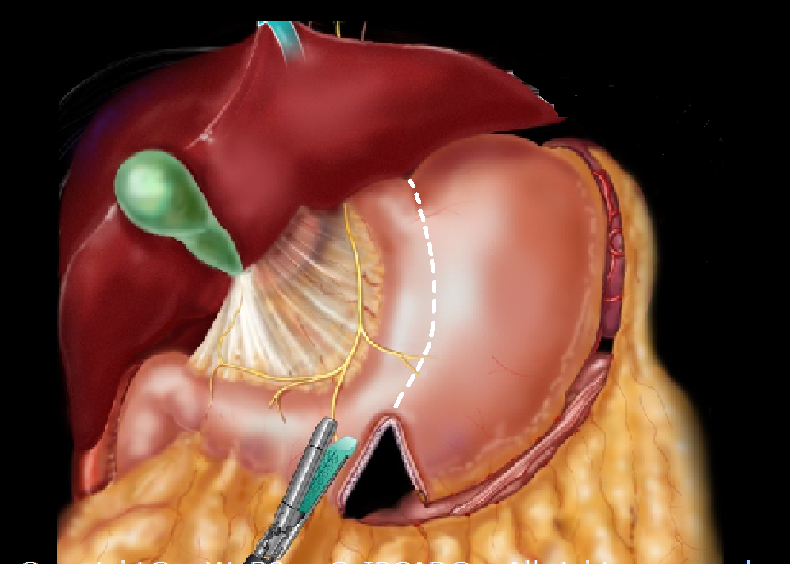
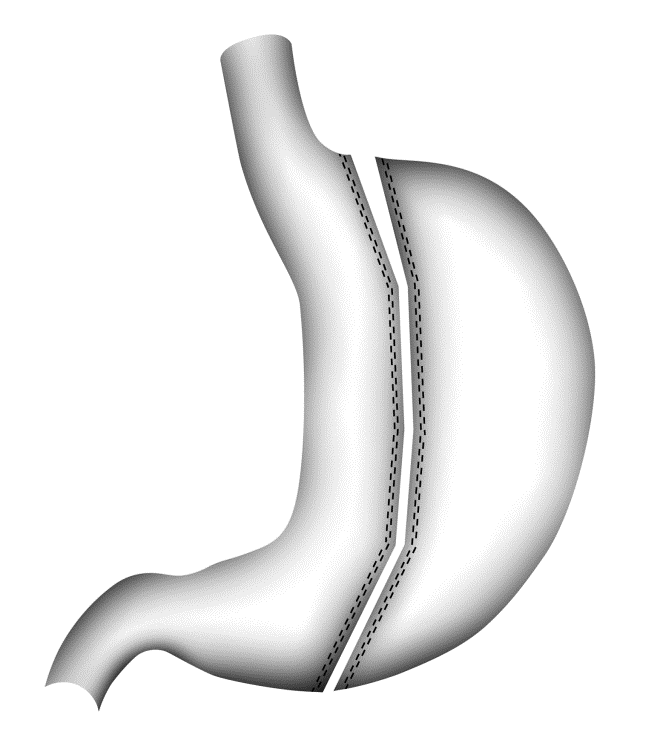
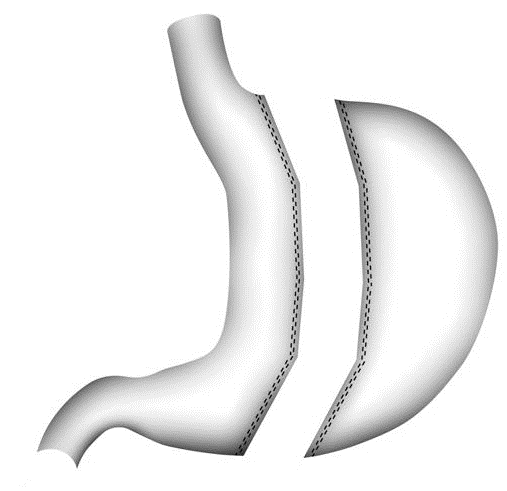
Schematic view of laparoscopic sleeve gastrectomy
Advantages of Sleeve gastrectomy (Pre-Surgical Preparation)
It is a surgical technique with very good results in moderately and severely obese patients.
Obesity-related co-morbidities such as hypertension, sleep apnea and diabetes improve by 70-80% after surgery.
This technique does not require enterotomy and religation.
There
will be no change in stomach functions, only the volume of the stomach
will decrease. Therefore, any type of food can be consumed normally,
though in small amounts.
The majority of patients lose 50% of their excess weight in the first 6 months after surgery.
As
a result of the removal of 75% of the stomach wall, the production of
Ghrelin hormone, which gives the feeling of hunger, is mostly eliminated
and therefore the feeling of hunger decreases.
Sleeve gastrectomy is a simpler operation than gastric bypass.
As
with procedures bypassing the small intestine, no malabsorption occurs
in minerals and vitamins, which may be important in elderly patients.
Dumping syndrome does not occur and sugar and sugary foods can be tolerated better.
As with the gastric band (stomach staple), there is no foreign device in the body.
It can be converted to other bariatric surgical operations when necessary.
Postoperative
late complications are rare. However, late complications can be seen at
a rate of 25% in gastric band and 10% in gastric bypass.
Disadvantages of sleeve gastrectomy :
This is an irreversible process.
Leakage (1%) and bleeding (2%) may occur in the stapler line due to stapling.
Preoperative preparations:
As
with other surgical operations, there are pre-operative preparations
that must be carried out carefully. Recommendations to you by your
doctor are usually as follows.
Advantages of sleeve gastrectomy
It is recommended to follow a diet for a week before surgery to reduce the fat around the liver.
Watery food intake for 48 hours before surgery.
In patients with constipation, it is necessary to clean the colon by taking magnesium citrate or Colyte before surgery.
Stop all medications you are taking unless your doctor has advised you to.
If
you are using any herbal medicine for headache or allergy or blood
thinner, it should be known before the operation. Especially 30% of
obese people have reflux disease. If so, surgical intervention for
reflux during the operation is performed in combination.
Stomach endoscopy is usually required before surgery. Gastric hernia, reflux disease, ulcer and tumor should be investigated.
Before
the operation, an upper abdominal ultrasound is definitely performed.
Generally, 30% of obese people have gallstones. If there is a
gallbladder stone, the gallbladder is removed during the surgery.
If
you smoke, you must definitely stop smoking a few weeks before the
surgery. Smoking slows wound healing. It increases the risk of
respiratory failure.
Laparoscopic
Sleeve Gastrectomy complication rates are the same as gastric band
(stomach staple), but significantly lower than Gastric Bypass. In
general, sleeve gastrectomy has two important complications as staple
line leak (1 0.2%) and bleeding (2 0.6%), apart from surgery and
anesthesia complications. Leakage is usually treated endoscopically with
a stent placed in the leak area. Any intervention for bleeding is
rarely required, it usually stops on its own. A blood transfusion may be
required.
“As of 2020, we have performed 1330
laparoscopic sleeve gastrectomy surgeries. Leakage occurred in three
patients (0.5%) and bleeding occurred in eight patients (0.6%). Leakage
was treated with endoscopic stenting. Blood transfusion was sufficient
for 6 out of 8 bleeding patients. In two patients, the bleeding was
stopped by surgery. We did not lose any patients"
Lifestyle and diet changes after surgery
Diet
and eating habits will change after surgery. You will need to drink
water more often (about 8 glasses of water per day), increasing by
10-20% if you exercise. Do not drink water or liquids with solid food.
With regard to food, the first two months will be the most difficult
period for you to adapt to your new stomach size. Due to the fact that
75% of the stomach is removed, patients can eat 1/4 of what they ate
before. During longer meal times (30-45 minutes for each meal), less
amount of food should be chewed more. When satiety is felt, it is
necessary to stop eating. Since you will eat very little at the
beginning, the meal should be 5 meals every day. The important thing is
to reduce the fat and carbohydrate ratio in the diet and to get enough
protein (1 g/kg) as a essential nutrients.
Vitamin deficiencies
are rarely seen after sleeve gastrectomy, unlike gastric bypass. Iron
deficiency anemia can be seen in 5% of cases, especially in women.
Female patients can become pregnant one year after surgery.
The benefits of stomach reduction surgery
The
vast majority of patients lose 60-80% of their pre-operative weight
within the first year. 75% of obesity-related problems such as
hypertension, diabetes, joint problems, high cholesterol and sleep apnea
improve or completely disappear after surgery. It is a great chance to
get rid of this disease or problem. Patients often feel that they have
come back to life. In addition, patients who have been disconnected or
distanced from social life due to obesity return to social life.
Diseases that occur due to obesity and disappear completely or improve considerably with the loss of excess weight.
OBESITY-RELATED DISEASE RECOVERY RATE (%)
Asthma 72
Gastroesophageal reflux disease (GERD) 60
Hypertension 70
High cholesterol level 77
Obstructive sleep apnea 80
Osteoarthritis of the knee and foot joints 75
Type 2 diabetes 70-85
Depression 75
There
are 5-6 surgical options in the treatment of morbid obesity. Sleeve
gastrectomy is one of the most commonly used methods. Your doctor will
recommend the most suitable surgical options for you after evaluating
your weight, comorbidities and surgical risks. Your life will change in a
few months. Do not miss the chance given to you to return to life and
live a life free from obesity.
Alternative Names
Bariatric Surgery – obesity surgery – laparoscopic sleeve gastrectomy – sleeve gastrectomy – tube stomach – stomach reduction